







• How to Treat Vertigo with Brandt-Daroff Exercises
• Understanding the Variables That Affect Vitamin D Status
• Benzocaine Warning from FDA Associated with the Use of Benzocaine
• Nitroglycerin for Osteoporosis?
• Phentermine plus Topiramate Leads to Significant Weight Loss at 1 Year
• Vitamin D Deficiency and Anemia in Older Men and Women
• Diet, Exercise, or Both in Obese Older Adults
• Diet Fuels Deficit; Cool Tool Tracks Nutrition Slide
• Dexamethasone Speeds Recovery in Pediatric Septic Arthritis
• Lumbar Disk Herniation: Older vs. Younger Patients
• Experts Issue Guidelines on Treating Painful Diabetic Neuropathy
How to Treat Vertigo with Brandt-Daroff Exercises
Vertigo is a disorder of the middle ear, caused by small crystals called ossicles that have colonized in a sensitive part of the inner ear. These crystals become displaced or misaligned, causing the dizziness of vertigo. Vertigo may be accompanied by tinnitus or a ringing in the ears. Frequently a physician who specializes in balance disorders and dizziness will perform The Epley or Semont maneuver to help settle the displaced crystals. The Semont maneuver is a calculated and rapid moving exercise, performed only by a doctor in the safety of a physician’s office. Brandt-Daroff exercises are similar to the Epley maneuver, but they can be done at home. These exercises can benefit anyone with dizziness, vertigo, imbalance, lightheadedness or faintness. They are safe and easy to perform
Instructions:
- Sit on the edge of the bed. You can also do this exercise on the floor or any flat surface.
- Turn your head left, at a 45-degree angle, so that your chin is halfway to your left shoulder. After you have turned your head to the left, lie down on your right side. While lying down, your head should still remain at a 45-degree angle, which is not against the flat surface, yet not pointing toward the ceiling. Stay in this position for 30 seconds. If you are experiencing vertigo, continue this position for one minute or until vertigo subsides.
- Sit up and into the normal sitting position as when you started. Remain sitting for 30 seconds.
- Turn your head right, at a 45-degree angle. Again, this angle would be turning your head so that your chin halfway meets with your right shoulder. After you have turned your head to the right, lie down on your left side. Remember that your head should remain at a 45-degree angle during this exercise. You should be facing halfway between the flat surface you're lying on and the ceiling. Stay in this position for 30 seconds. If you are experiencing vertigo, continue this position for one minute or until vertigo subsides.
- Return again to the sitting position on the edge of your bed. Stay sitting for 30 seconds. This exercise completes one set. Complete five repetitions in the morning, five repetitions at noon and five repetitions in the evening.
Rate of Success:
Brandt-Daroff exercises should be performed until you have reached 52 sets over a period of two to three weeks. Most people receive complete relief from dizzy symptoms after 30 sets. However, one-third of patients will have symptoms reoccur within a year. If this happens, perform one set daily until symptoms are relieved
Warning:
If you have been treated at the doctor's office for the Epley or Semont maneuver, do not perform these exercises until a physician instructs you to do so
http://www.ehow.com/how_2303034_treat-vertigo-brandt_daroff-exercises.html
Youtube video demonstrating this exercise: http://www.youtube.com/watch?v=hhinu_oU_hM
Top of Page
Acta Derm Venereol 2011 Mar; 91:115
Understanding the Variables That Affect Vitamin D Status
Location, pollution, weight, and health affect your ability to absorb, store, and make use of vitamin D.
It has been estimated that 30% of the U.S. population (and 9% of U.S. children) are vitamin D insufficient or deficient. Among those at risk for vitamin D deficiency are people who are older, live at higher latitudes, or have darker skin, and those whose religious observance requires them to cover large areas of skin. A recent review provides additional information on factors that affect an individual's vitamin D status.
Exposure. The authors indicate that during prolonged exposure to ultraviolet B (UVB; 290–320 nm) radiation, only about 10% to 15% of 7-dehydrocholesterol is converted to vitamin D3 because of its breakdown to inactive compounds. Several environmental factors influence vitamin D metabolism. For example, in certain regions of the world, the decline in stratospheric ozone has increased the amount of vitamin D3-effective UVB radiation by 15%. Vitamin D synthesis is tempered by cloud cover, which can reduce terrestrial UVB to 1% of clear-sky levels, and by pollutants generated by the incomplete combustion of fossil fuels. Although in theory, regular sunscreen use would reduce vitamin D levels, clinical studies of this hypothesis have yielded conflicting results.
Availability. Because it is a lipid soluble molecule, vitamin D3 is stored in adipose tissue. The obese tend to have lower vitamin D levels, presumably because of adipose tissue sequestration. Circulating vitamin D levels are also influenced by gastrointestinal (GI) absorption and by enzymatic activity in the kidney and liver. Conditions that affect the GI tract (e.g., cystic fibrosis, Crohn disease, gastric bypass), kidney (chronic renal failure), or liver (cholestatic and severe parenchymal liver disease) can decrease vitamin D levels.
Drug Effects. Medications that adversely affect vitamin D status include phenobarbital, phenytoin, carbamazepine, rifampicin, and antiretrovirals. On the other hand, activated macrophages in granulomatous diseases (sarcoid, tuberculosis, systemic fungal infections, berylliosis) can cause extrarenal metabolism of vitamin D, resulting in hypercalcemia.
Comment: The Institute of Medicine recently published its recommendations on vitamin D supplementation. Physicians must consider all factors that influence vitamin D metabolism when advising their patients. For example, individuals with vitamin D deficiency, such as the elderly, may benefit from less-aggressive recommendations regarding sunscreen use if they do not have extensive actinic damage. On the other hand, it may be inadvisable to use phototherapy for patients at risk for hypercalcemia.
— Craig A. Elmets, MD Published in Journal Watch Dermatology April 15, 2011
Citation(s): Tsiaras WG and Weinstock MA. Factors influencing vitamin D status. Acta Derm Venereol 2011 Mar; 91:115.
http://www.ncbi.nlm.nih.gov/pubmed/21384086?dopt=Abstract
Top of Page
Benzocaine Warning from FDA Associated with the Use of Benzocaine
A drug safety communications about a serious adverse effect associated with the use of over-the-counter (OTC) benzocaine gels, sprays, and liquids applied to the throat and gums to reduce pain has been issued by the FDA.
The warning involves the use of benzocaine which is associated with methemoglobinemia, and in the most severe cases, can result in death. Methemoglobinemia has been reported with the use of all strengths of benzocaine gels and liquids, including concentrations as low as 7.5%. The cases reported occurred mainly in children aged 2 years or younger who were treated with benzocaine gel for teething.
The recommendations are that parents and caregivers should not use OTC benzocaine products on children under 2 years of age, except under the advice and supervision of a healthcare professional. If benzocaine products are used, it should be used sparingly and only when needed, but not more than 4 times a day.
FDA issued a public health advisory warning in 2006 about methemoglobinemia with the use of benzocaine sprays during medical procedures. FDA has reportedly received notice of 72 new cases of methemoglobinemia, including 3 resulting in death, associated with the use of benzocaine sprays, bringing the total to 319 cases.
"While FDA's announcement notes very rare but serious instances of methemoglobinemia . . . these products are safe when used as directed for the large majority of consumers," according to a statement prepared by the Consumer Healthcare Products Association, in Washington, DC.
http://www.modernmedicine.com/modernmedicine/Clinical+News/FDA-warns-about-a-serious-adverse-effect-associate/ArticleStandard/Article/detail/715831?context
CategoryId=40137
Top of Page
JAMA 2011 Feb 23; 305:800
Nitroglycerin for Osteoporosis?
A Canadian trial showed favorable skeletal effects, but headaches are a concern.
Nitric oxide inhibits osteoclast activity, and intermittent use of nitroglycerin (NTG) can improve skeletal health outcomes in menopausal women. In a single-center blinded trial, Canadian investigators randomized 243 menopausal women (mean age, 62; 92% white) who did not have osteoporosis and were not taking medications known to affect bone-mineral density (BMD) to daily NTG ointment (15 mg) or placebo for 24 months.
In the NTG group, percent change in BMD from baseline gradually increased in magnitude during follow-up. At 2 years, compared with women who received placebo, those who received NTG experienced greater increases in lumbar spine BMD and total hip BMD relative to baseline (difference in percent change from baseline, 6.7% and 6.2%, respectively; P<0.001 for either site). Treatment with NTG was associated with augmentation of bone strength and formation and attenuation of resorption. Serious adverse events occurred with similar frequency in the two study groups. However, 5.6% of women in the NTG group and 1.7% of those in the placebo group discontinued study treatment during the first year because of headaches. Among women who continued treatment for 24 months, headaches were reported by 35.0% of NTG recipients versus 5.4% of placebo recipients.
Comment: This trial shows that transdermal administration of NTG for 2 years increased BMD as well as bone strength. Intriguingly, the favorable skeletal effects of NTG seemed to develop over time; this contrasts with the effects of other agents currently indicated for fracture prevention. The most important adverse effect was headaches, which might limit the appeal of NTG should the drug be approved for fracture prevention. A larger longer-term trial to assess NTG's efficacy in preventing fractures would be appropriate; in addition, strategies to minimize NTG-associated headaches while maintaining the drug's skeletal benefits should be evaluated.
— Andrew M. Kaunitz, MD Published in Journal Watch Women's Health March 10, 2011
Citation(s): Jamal SA et al. Effect of nitroglycerin ointment on bone density and strength in postmenopausal women: A randomized trial. JAMA 2011 Feb 23; 305:800.
http://www.ncbi.nlm.nih.gov/pubmed/21343579?dopt=Abstract
Top of Page
The Lancet, Early Online Publication, 11 April 2011 doi:10.1016/S0140-6736(11)60205-5
Phentermine plus Topiramate Leads to Significant Weight Loss at 1 Year
A combination of phentermine and topiramate appears to be an effective obesity treatment, according to a phase III, industry-conducted trial published in the Lancet.
Some 2500 patients who were overweight or obese and had at least two comorbidities were randomized to placebo or low- or high-doses of phentermine plus topiramate. All patients received diet and lifestyle counseling. At 56 weeks, patients in the treatment groups lost more weight than controls (high-dose, 10.2 kg; low-dose, 8.1 kg; placebo, 1.4 kg). A higher proportion of patients in the treatment groups also achieved 10% weight loss (high-dose, 48%; low-dose, 37%; placebo, 7%).
Patients in the treatment groups reported higher rates of dry mouth, constipation, and paresthesia. In addition, a dose-related increase was observed in depression- and anxiety-related adverse events.
http://www.thelancet.com/journals/lancet/article/PIIS0140-6736%2811%2960205-5/abstract
Top of Page
Blood 2011 Mar 10; 117:2800.
Vitamin D Deficiency and Anemia in Older Men and Women
VDD was associated with specific subtypes of anemia, particularly anemia of inflammation.
Recent studies have shown that more than one third of middle-aged and older individuals have vitamin D deficiency (VDD) and that 10% of people ≥65 have anemia. To determine whether VDD is associated with anemia in older adults, investigators analyzed hemoglobin, vitamin D, and other data for nearly 5000 participants (age, ≥60) in the National Health and Nutrition Examination Survey. VDD was defined as serum levels <20 ng/mL; anemia was defined as hemoglobin levels <13 g/dL in men and <12 g/dL in women.
Anemia was more prevalent in individuals with VDD than in those without VDD (12.3% vs. 7.4%; odds ratio, 1.78; P< 0.001); this association remained after adjustment for age, sex, and race/ethnicity (OR, 1.47; P=0.02). VDD was more prevalent in individuals with anemia of inflammation (AI) than in those without anemia (56.0% vs. 33.3%; P=0.008); VDD was also more prevalent in those with anemia of nutrient deficiency (47.7%; P=0.001) and anemia of chronic kidney disease (37.1%; P=0.04), but not unexplained anemia (33.0%), compared with those without anemia. An association of VDD with AI versus unexplained anemia persisted after adjustment for age, sex, and race/ethnicity (relative risk ratio, 2.47; P=0.043). Blacks were more likely to have VDD than whites, and blacks were overrepresented among people with AI; after adjustment for age and sex, blacks had a sevenfold greater risk of having AI than whites.
Comment: AI is characterized by disordered iron-limited erythropoiesis and elevated levels of inflammatory cytokines. The association of AI with VDD suggests that vitamin D might suppress inflammatory pathways that contribute to the development of AI. Whether VDD plays a causal role in the anemia or simply augments the effects of inflammation on erythropoiesis will require further study.
— David Green, MD, PhD Published in Journal Watch Oncology and Hematology April 12, 2011
Citation(s): Perlstein TS et al. Prevalence of 25-hydroxyvitamin D deficiency in subgroups of elderly persons with anemia: Association with anemia of inflammation. Blood 2011 Mar 10; 117:2800.
http://www.ncbi.nlm.nih.gov/pubmed/21239700?dopt=Abstract
Top of Page
N Engl J Med 2011 Mar 31; 364:1218
Diet, Exercise, or Both in Obese Older Adults
Combining dieting and exercise improved physical performance — but so did dieting or
exercise alone.
Because obesity predisposes older adults to disability, we often advise such patients to diet and get exercise. To determine the relative contributions of these two interventions, researchers randomized 107 obese older adults (age, ≥65; body-mass index, >30 kg/m2) with mild-to-moderate frailty to receive a diet intervention, exercise intervention, both, or neither. The diet intervention consisted of individualized weight-loss diets targeted to 10% reduction of baseline weight and weekly group sessions with dieticians. The exercise intervention consisted of 90-minute, thrice-weekly group sessions that included aerobic exercise and resistance training.
At 1 year, mean weight loss was about 9 kg in both the diet-only and diet–exercise groups but was negligible in the exercise-only and control groups. Mean improvement on a 9-task, 36-point physical performance test (the primary outcome) was best in the diet–exercise group (5.4 points), intermediate in the exercise-only and diet-only groups (4.0 and 3.1 points, respectively), and negligible in the control group.
Comment: Unsurprisingly, a combination of dieting plus exercise improved physical performance more than dieting or exercise alone. However, the exercise-only intervention improved physical performance nearly as much as the combined intervention; that's an important message to convey to older patients who successfully engage in exercise but are frustrated by inability to lose weight. The interventions in this study were labor-intensive (from the healthcare system's perspective) and required substantial commitment (from the patient's perspective).
— Allan S. Brett, MD Published in Journal Watch General Medicine April 12, 2011
Citation(s): Villareal DT et al. Weight loss, exercise, or both and physical function in obese older adults. N Engl J Med 2011 Mar 31; 364:1218. (http://dx.doi.org/10.1056/NEJMoa1008234)
http://www.ncbi.nlm.nih.gov/pubmed/21449785?dopt=Abstract
Top of Page
Article from Vital Choices Newsletter
April 14, 2011
(http://newsletter.vitalchoice.com/e_article002077613.cfm?x=bjlbj2k,b1h1R7NC)
Diet Fuels Deficit; Cool Tool Tracks Nutrition Slide
Costs of diet/lifestyle-driven disease equal size of proposed budget cuts; New interactive diagram shows steady decline in American diets over four decades
by Craig Weatherby and Randy Hartnell
New York Times food writer Mark Bittman deserves kudos for drawing a straight line between the bitter budget fight in Congress and a major source of the nation’s growing tide of red ink.
In his April 14 column, titled “How to Save a Trillion Dollars”, he includes this sobering comment by pediatrician David Ludwig, M.D., author of Ending the Food Fight:“… the $4 trillion that the Republicans want cut over a decade is about the same as the projected costs of diabetes over that same period.” (Bittman M 2011). And, as Bittman notes, the American Heart Association editorial board estimates costs in the U.S. from cardiovascular disease “will triple by 2030, to more than $800 billion annually. Throw in about $276 billion of what they call ‘real indirect costs,’ like productivity, and you have over a trillion.” (Bittman M 2011). He adds that within 10 years, diabetes will cost Americans about $500 billion a year, even though it’s almost always preventable with healthy diets and moderate exercise.
A very substantial portion of heart and diabetes care costs are borne by taxpayers, since both diseases occur most frequently among the retired and the poor, who are served by Medicare and Medicaid respectively. Of course, the remaining healthcare costs not borne by U.S taxpayers come out of the pockets of companies and individuals, putting a drag on the economy while limiting personal choices and retirement savings. Bittman made that larger economic point as well: “For the first time in history, lifestyle diseases like diabetes, heart disease, some cancers and others kill more people than communicable ones. Treating these diseases — and futile attempts to ‘cure’ them — costs a fortune, more than one-seventh of our GDP.”
We recommend his blog post highly … click here to read “How to Save a Trillion Dollars”.
Interactive “American-diets-over-time” chart paints unhealthy picture
We just came across a nifty, interactive diagram that puts America’s grossly imbalanced diet on display in a graphic, disturbing way ... and serves to underscore Mark Bittman’s points. The diagram shows which food groups have provided the average American’s calories, every year from 1970 through 2008. The chart presents annual calorie-consumption numbers by food type.
Click here to launch the interactive version:
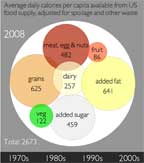
The diagram shows which food groups have provided the average American’s calories, every year from 1970 through 2008.
It’s based on USDA data on the volumes of various foods produced, and the amounts lost due to spoilage and waste, to provide a best estimate of the foods actually consumed.Usefully, the diagram includes the numbers of calories provided by added fats and added sugars.As you slide the line from left to right, you see American diets getting less healthy over time … with more and more calories coming from added sugars, added fats, and grains … most of which were would have been consumed in the form starchy, nutrient-poor refined flour. We’re impressed with the visual impact of this diagram, created as part of a partnership between Civil Eats and the UC Berkeley Graduate School of Journalism’s News21 course on food reporting. The diagram is introduced by journalist Andrea Jezovit, who notes that it shows calorie intake rose 23.3 percent from 1970 to 2008. Ouch!
Sources: Bittman M. How to Save a Trillion Dollars. The New York Times. April 12, 2011. Accessed at http://opinionator.blogs.nytimes.com/2011/04/12/how-to-save-a-trillion-dollars/; Jezovit A. Where Do Americans Get Their Calories? (Infographic). Civil Eats. Accessed at http://civileats.com/2011/04/05/where-do-americans-get-their-calories-infographic/
Top of Page
J Pediatr Orthop 2011 Mar; 31:211
Dexamethasone Speeds Recovery in Pediatric Septic Arthritis
A randomized study confirms a benefit from corticosteroid treatment.
Septic arthritis is an acute, painful infection that can lead to sequelae of the affected joints, and dexamethasone has been associated with good clinical responses in children with this condition. In a double-blind, placebo-controlled study, researchers in Israel randomized 49 children (age range, 6 months to 18 years) with septic arthritis to receive intravenous (IV) dexamethasone (0.15 mg/kg every 6 hours for 4 days) or placebo beginning before or within 2 hours of antibiotic treatment.
Patient characteristics, affected joints, bacterial pathogens, and laboratory parameters were comparable in the two groups. All joints except septic hips were treated medically. Dexamethasone was associated with significantly faster resolution of fever (1.7 vs. 2.8 days), faster resolution of pain (7.2 vs. 10.8 days), and shorter duration of IV treatment (9.9 vs. 12.6 days). All 29 patients (17 in the dexamethasone group) who were followed up after 1 year had excellent long-term outcomes, and none had adverse effects or residual symptoms.
Comment: This study confirms a benefit from corticosteroids in pediatric septic arthritis. A 2003 study demonstrated significantly decreased residual dysfunction at 6 and 12 months in children treated with dexamethasone (given prior to antibiotics) compared with placebo (Pediatr Infec Dis J 2003; 22:883). Although the number of methicillin-resistant Staphylococcus aureus (MRSA) infections in both studies was relatively small, I believe outcomes in children with MRSA infections would be similar. I definitely recommend adding corticosteroids to antibiotic treatment for pediatric septic arthritis. Our institution is actively working with our orthopedic colleagues to implement the practice of adding steroids to the treatment regimen for children with septic arthritis to improve both short- and long-term morbidity.
— Peggy Sue Weintrub, MD Published in Journal Watch Pediatrics and Adolescent Medicine
April 6, 2011
Citation(s): Harel L et al. Dexamethasone therapy for septic arthritis in children: Results of a randomized double-blind placebo-controlled study. J Pediatr Orthop 2011 Mar; 31:211.
http://www.ncbi.nlm.nih.gov/pubmed/21307717?dopt=Abstract
Top of Page
J Am Geriatr Soc 2011 Mar; 59:423
Lumbar Disk Herniation: Older vs. Younger Patients
Outcomes of nonsurgical treatment were similar, regardless of age.
We tend to attribute lumbosacral radicular symptoms to herniated disks in young and middle-aged patients and to degenerative spinal stenosis in older patients. However, symptomatic disk herniation also occurs commonly in older patients. In a prospective cohort study from an outpatient spine clinic in Boston, researchers compared outcomes among older and younger patients with recent-onset lumbosacral radicular pain (and corresponding herniated disks on magnetic resonance imaging) who were treated nonsurgically.
Of 133 consecutive patients encountered during 1 year, 44 (33%) were older (age, ≥60; mean age, 68), and 89 were younger. Treatment modalities — including physical therapy, chiropractic, epidural steroid injections, and oral medications — were prescribed with similar frequency in the two age groups. Interestingly, the older group had somewhat faster improvement in leg and back pain than did the younger group. By 6 months, however, the degree of clinical improvement (according to back pain, leg pain, and disability scores) was virtually identical in younger and older patients. For example, mean leg pain scores dropped from about 7 to 2 (on a 10-point scale) in both groups.
Comment: This study suggests that disk herniation is not unusual as a cause of lumbosacral radicular symptoms in older people and that outcomes with nonsurgical treatment are roughly similar in older and younger patients.
— Allan S. Brett, MD Published in Journal Watch General Medicine March 29, 2011
Citation(s): Suri P et al. Nonsurgical treatment of lumbar disk herniation: Are outcomes different in older adults? J Am Geriatr Soc 2011 Mar; 59:423.
(http://dx.doi.org/10.1111/j.1532-5415.2011.03316.x)
http://www.ncbi.nlm.nih.gov/pubmed/21391933?dopt=Abstract
Top of Page
Experts Issue Guidelines on Treating Painful Diabetic Neuropathy
Pregabalin should be offered for the treatment of painful diabetic neuropathy (level A evidence), according to new guidelines from the American Academy of Neurology, American Association of Neuromuscular and Electrodiagnostic Medicine, and the American Academy of Physical Medicine and Rehabilitation.
Among the other recommendations (level B or C evidence), published in Neurology:
- Anticonvulsants: Gabapentin and valproate should be considered for treatment, while evidence is insufficient to recommend for or against using topiramate. Oxcarbazepine, lamotrigine, and lacosamide "probably" should not be given.
- Antidepressants: Amitriptyline, venlafaxine, and duloxetine should be considered, and venlafaxine can be added to gabapentin. Evidence is insufficient to recommend for or against other agents (e.g., fluoxetine).
- Opioids: Dextromethorphan, morphine sulfate, tramadol, and oxycodone should be considered.
- Other pharmacologic agents: Capsaicin or the Lidoderm patch may be considered.
- Nonpharmacologic methods: Electrical stimulation should be considered, while magnetic field treatment is not recommended.
http://www.neurology.org/content/early/2011/04/08/WNL.0b013e3182166ebe.full.pdf+html
Top of Page
